Much crucial detail from the inquest into the tragic death of Savita Halappanavar is emerging in the media, which is being seized upon and manipulated by opponents of Ireland’s pro-life laws as well as those with an anti-Catholic or militant secular agenda.
The inference is clear – Catholic dogma is responsible for the death of a pregnant woman from sepsis, as evidenced, according to one tweeter, by the presence of a religious statue outside of Galway University College Hospital and the fact that many of the wards are named after saints. Something of a non-sequitur. Clearly the presence of religious symbolism, a reflection of Ireland’s cultural heritage, is indicative that patients can expect a substandard level of care, where medically unsafe and morally dubious dogma overrides the best clinical interests of the patients. Anyone attending St Thomas’s or Bart’s hospitals in London had better be on their guard!
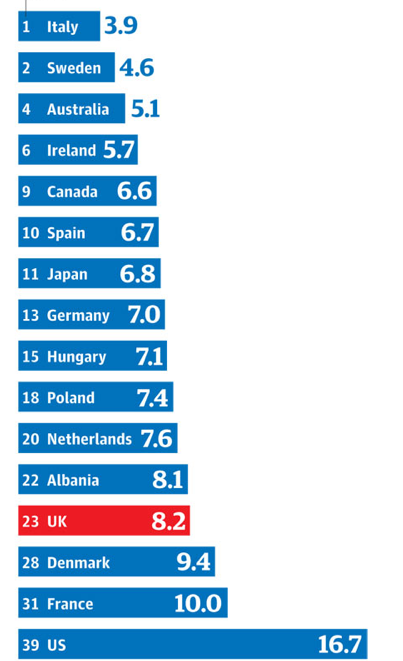
Let’s start with the stats.
Here’s a table showing the maternal mortality ratio, the number of maternal deaths per 100,000 live births from the Guardian’s datablog, where ‘facts are sacred’.

So, the one of the highest rates of maternal mortality occurs in the US which rather disproves the claim that liberal abortion legislation is safer for women. Ireland, that country where women are deprived of abortion, has one of the lowest maternal death rates in the world, official stats show that on average 4,000 women in the Republic travel to the UK for an abortion every year, a figure that has been steadily decreasing from a high of 6,600 in 2001, so the blame for the UK’s relatively poor performance in the area of maternal health care, can hardly be explained away as being an Irish export. Pro-life Chile has the lowest maternal death rate in Latin America and Poland, another pro-life country also fares well.
Furthermore, more than 100 mothers have died in childbirth in London in the last five years, twice the rate of that of the rest of the country. Whilst we are all screaming about the first maternal death in 17 years at a hospital in Galway, where is the outrage about the lamentable situation in the UK, due to a desperate shortage of midwives? Surely anyone who identifies themselves as ‘pro-woman’ should be demanding to know how the government intends to remedy this increasing problem, aside from disincentivising those who may want more than two children?
Whilst on the subject of outrage, where were the candlelit vigils and expressions of anger over the death of Jessie-Maye Barlow, God rest her soul, the 19 year old mother of one, who died from septic shock following an abortion in September 2012, the inquest acknowledging that BPAS had not followed up on their aftercare and thus the fact that Jessie-Maye had failed to pass all the ‘products of conception’ was missed, leading to her death? Where were the protestations of anger that a beautiful young mother of one, with her entire life in front of her died as a direct result of medical negligence on behalf of an abortion clinic that was too busy to follow basic protocols regarding patient care?
Sepsis
Savita Halappanavar died from sepsis. According to the Royal College of Obstetricians and Gynaecologists, between 2003 and 2005 there were five maternal deaths in the UK of pregnant women from sepsis, with a baby under 24 weeks gestation. “Sadly, substandard care was identified in many of the cases, in particular lack of recognition of the signs of sepsis and a lack of guidelines on the investigation and management of genital tract sepsis. Between 2006 and 2008 sepsis rose to be the leading cause of direct maternal deaths in the UK, with deaths due to group A streptococcal infection (GAS) rising to 13 women. Severe sepsis with acute organ dysfunction has a mortality rate of 20 to 40%, which increases to 60% if septic shock develops. Studies in the non-pregnant population have found that the survival rates following sepsis are related to early recognition and initiation of treatment.”
In 2012 the RCOG published green top guidelines for treatment of sepsis in pregnancy. The guidelines state
The signs and symptoms of sepsis in pregnant women may be less distinctive than in the non- pregnant population and are not necessarily present in all cases; therefore, a high index of suspicion is necessary.
The diagnosis of sepsis must be confirmed by blood cultures and early swift administration of broad spectrum antibiotics are the key to the survival of the patient, alongside regular monitoring.
Crucially and unfortunately, this did not happen in the case of Savita, who was admitted into the hospital on the evening of Sunday 21st October. Blood tests that were taken that night, which were never followed up on, showed an elevated white blood cell count which would have been one of the key indicators that infection and indeed sepsis was present.
Whilst oral antibiotics appear to have been started on the Monday night, following the spontaneous rupture of membranes, an infection of the severity of Savita’s would have required intravenous administration. The consultant obstetrician has described the situation as a systems failure on multiple counts, not only were the blood results not followed up on, but also, the vital regular observations which may have alerted the staff to the presence of an infection sooner, were not carried out at regular intervals throughout the night, which is why the infection was only picked up in the early hours of the Wednesday morning, after Savita had taken a dramatic turn for the worse, a doctor who had come to check on her on the Tuesday evening, saw she was asleep and so left her. Once Savita’s membranes had ruptured (in the early hours of Monday morning) then she should have been checked every 4 hours for signs of infection.
The RCOG guidelines state that all staff should be aware of the signs and symptoms of potential sepsis and the rapid and potentially lethal course of the disease, which is often less distinctive in pregnant women. Therefore whilst one can reasonably assume that care was lacking, notably in the failure to follow up on the results of the blood tests, the narrative that University College Hospital Galway were knowingly refusing to treat a woman with a severe and life-threatening infection in order to prioritise the life of her baby, due to Catholic dogma reflected in the law, is an erroneous one. As the consultant testified, had they known about the sepsis or infection, they would have intervened much sooner, however Savita’s symptoms did not physically manifest until the early hours of Wednesday morning, over 48 hours since she was first admitted, whilst the signs may have been present, i.e. a slightly elevated temperature and raised pulse rate, this could also have been due to other factors, such as anxiety and it is only with hindsight and in the light of the missing bloodwork, that this can be identified as being the start of the infection.
Speaking to the inquest, Savita’s husband has reported that doctors seemed nonchalant on Tuesday, certainly there was no cause for concern, or reason to think that her life might be at stake.
Abortion to treat Sepsis – a red herring
Savita’s sepsis stemmed from an antibiotic resistant strain of E-coli, an issue that is in itself concerning. Pathology has indicated that the infection most likely originated in her urinary tract and tallies with the backache that she complained of, prior to admission to hospital. Aborting the baby would not have cured Savita of her infection and indeed in these situations, surgery is to be avoided if at all possible, as it runs the very real risk of spreading the infection further and causing death.
Whilst the hospital had failed to spot the infection, they had noted that an inevitable miscarriage was taking place. Savita, understandably, was very distressed, and wished for her ordeal to be over, as opposed to the interminable wait for nature to take its course and allegedly requested an abortion on the Tuesday morning, following the ultrasound to determine the baby’s progress.
Upon admission to hospital on the Sunday night, it was noted that no cervix could be felt, hence Savita was fully dilated and hence the premature delivery of the baby was imminent, which would mean that the baby would not survive. Later on, her membranes ruptured, meaning that the protective sac of fluid surrounding the baby completely drained, a situation which would likely result in the death of the baby and spontaneous natural delivery.
This is where the confusion sets in, which is being exploited to the max by the abortion lobby. Firstly, that Savita was fully dilated, was as a direct result of the infection which was in her urinary tract. The unborn baby was in a sterile sac of waters and therefore not the cause of the infection. The dilated cervix did not cause her infection either. An open or dilated cervix will not cause an infection, as any woman who has ever had more than one baby, or indeed a smear test will testify. Once you have had a baby, the cervix never fully closes. When I was pregnant with my eldest child, I was dilated by 2cm for a good week before I delivered. An open cervix does not make one more ripe for infection.
The infection risk is posed when the membranes or waters have ruptured, normally hospitals will be wanting a woman to deliver within 48 hours of this occurring in order to minimise risk of infection to the newborn baby. Clearly in Savita’s case this would not have applied, but if her waters broke on the Sunday night, it was not unreasonable for no action to have been taken on the Tuesday, the medics obviously thought that delivery or natural miscarriage would take place swiftly and that conservative management was the safest option in the circumstances.
Whilst Savita may have requested a termination, this may well not have been in her best medical interests.
The unborn baby was not the cause of the sepsis and so there was no good reason to terminate it as Savita’s life did not seem to be at risk. Dr. Hema Divakar, President-elect of the Federation of Obstetric and Gynaecological Societies of India speaking to the Hindu Times said:
“Delay or refusal to terminate the pregnancy does not in itself seem to be the cause of death. Even if the law permitted it, it is not as if her life would have been saved because of termination. Severe septicaemia with disseminated intravascular coagulation (DIC), a life-threatening bleeding disorder which is a complication of sepsis, major organ damage and loss of the mother’s blood due to severe infection, is the cause of death in Savita’s case. This is what seems to have happened and this is a sequence which cannot be reversed just by terminating the pregnancy.”
Catholicism and the law
It seems to me that there is something of a cop-out or buck passing exercise going on here. Dr Katherine Astbury, the doctor in charge of Savita’s care, told the inquest that in Ireland it is not legal to terminate a foetus on the grounds of poor prognosis for the foetus, but also admitted that she did not once clarify the legal situation with her colleagues or think to do so.
The law in Ireland does not prevent a termination from being carried out, if the life of the mother is at risk and as Dr Astbury testified, had she known the severity of the situation she would have intervened earlier, although from what we know now, an abortion could well have made the situation a lot worse. It seems obvious, that Dr Astbury perhaps sought to take shelter in the law as opposed to exercise her own moral and clinical judgement. No law can be formulated that will cover all the possible permutations and complications that might arise from real-life pregnancy management and so doctors can’t ever be entirely freed from having to make theraputic and ethical decisions. Whilst doctors might have to work within the law, they also need to exercise clinical judgement which will invariably and inevitably involve ethics.
The law in Ireland is clear, section 21:4 of the Medical Council Guide for Registered Practitioners says this:
“In current obstetrical practice, rare complications can arise where therapeutic intervention (including termination of a pregnancy) is required at a stage when, due to extreme immaturity of the baby, there may be little or no hope of the baby surviving. In these exceptional circumstances, it may be necessary to intervene to terminate the pregnancy to protect the life of the mother, while making every effort to preserve the life of the baby.”
So there was no legal reason why the pregnancy could not have been terminated were Savita’s life deemed to be at risk. One has to wonder why Dr Astbury couched her response to Savita’s request in purely legal terms? This was not simply about what the law proscribed, but medically speaking, conservative management of delivery is the safest approach, in the absence of any other pressing clinical factors. Theatre was obviously felt to be unnecessary at this stage, the cervix had dilated, the membranes had ruptured, delivery could not be far off, there was still a foetal heartbeat, the prognosis for the baby was poor, but there was no pressing need to abort medically, as well as legally. Why were the medical reasons not explained to her – that it was presented purely in legal terms seems to be a total failure of communication and gave the Halappanavar’s the impression that best clinical practice was being hampered by the law. The only people qualified to judge on whether or not an abortion should be performed were the doctors, not the lawyers and if any conflict had been perceived, why was this not instantaneously taken up with the hospital’s legal team, who would have been well versed in the ethics.
The Irish Catholic Bishops, responding to the case, said this:
The Catholic Church has never taught that the life of a child in the womb should be preferred to that of a mother. By virtue of their common humanity, a mother and her unborn baby are both sacred with an equal right to life.
– Where a seriously ill pregnant woman needs medical treatment which may put the life of her baby at risk, such treatments are ethically permissible provided every effort has been made to save the life of both the mother and her baby.
Which is why the conjecture over potential situations coming from all sides is unhelpful. Catholic teaching is very clear. Mother and baby have an equal right to life, whilst a baby must never be directly killed in order to save the life of a mother (and I cannot envisage a single situation where that would be necessary), a mother may receive treatment such as in the case of an ectopic pregnancy or a cancer diagnosis, which may put the life of her unborn baby at risk, or may end a baby’s life as an indirect consequence.
‘This is a Catholic country’
This was the comment made by Ann Maria Burke, a midwife manager, in response to a conversation with Savita, who stated that in India, a Hindu country, an abortion would be possible. Now is not the place to discuss India’s abortion record, especially when it comes to baby girls or how that reflects Hinduism, which treats all life as sacred, but as Ms Burke now admits, the remark was regrettable and had nothing to do with medical care. The remark perhaps smacks of racism, or was made in the context of a general conversation pertaining to religious and cultural attitudes, but tellingly the midwife was not directing the care of Mrs Halpannavar, nor was she dictating hospital policy. She was trying to explain the reason behind Ireland’s pro-life laws, which whilst they might stem from and be in accordance with Ireland’s Catholic history, do not indicate that Ireland is currently a country that is governed by those in accordance with the Catholic Church, quite the opposite Enda Kenny the current Taoiseach is doing all that he can to put distance between himself and the Vatican. Moreover Catholic moral theology would not sanction the delivery of a non viable baby as a direct cure for a pregnant woman, and is therefore slightly at odds with the letter of Irish law.
Conclusion
Had the initial blood tests been followed up on, and 4 hourly observations undertaken, then perhaps the tragedy may not have unfolded in the way that it did. What seems clear is that the infection was present upon admittance to hospital and that it is unlikely that an abortion would have cured the infection and potentially could have hastened Savita’s death. The unborn baby could not have been the source of the infection and by the time that the infection was noted, things had already progressed too far. The infection was obviously incredibly aggressive and Savita’s condition deteriorated so rapidly on Wednesday 24 October, that the decision as to whether or not to abort became moot. According to the inquest, septic shock was diagnosed at 1.20pm, two hours later, Savita’s already dead baby was delivered in theatre, so the conservative approach would have been the correct one, nature had taken its course swiftly, within the normal 48 hour window.
There is no indication that the hospital was ignoring the plight or symptoms of a critically ill woman with sepsis in order to rigorously follow the letter of the law regarding her unborn baby, when the law already allowed for an abortion to take place in these circumstances. Until the early hours of Wednesday morning, there was no obvious manifestation of infection, to those caring for her. It was only then that seriousness of the situation became glaringly apparent.
The issues here are about an awareness of sepsis. That is what Parveen Halappanavar, Savita’s husband should be angry about. This is the issue that he should fight for in his wife’s memory, as well as suing the hospital for their negligence in following up on her blood tests. Understandably he wanted his wife’s distress to be alleviated by an abortion, a procedure that may well not have been in her best interests either physically or emotionally. That the hospital could only explain this in legal terms is as great a dereliction of care and duty as it was not to have chased her blood results or carried out her observations.
Ireland’s abortion laws may change as a result, unborn babies will die and no action will be taken to address the urgent problem of sepsis diagnoses, nor indeed the worrying spread of ESBL bacteria that killed Savita. Abortion won’t cure sepsis or aid its diagnosis. It may however mean that more women and babies are exposed to the deadly bacteria. Savita’s memory deserves better.