Miserable sinner, aspiring saint, propensity towards melodrama and general bawdiness, probably not the best example of holiness, but trying nonetheless. A woman who wears her heart on her sleeve and talks a great deal of nonsense. You're not going to gain any profound insight from my ramblings and fulminations, but you're welcome to share the journey.
So whilst ordinary lay Catholics are fighting tooth and nail in order to keep abortion out of Ireland, whilst GPs are finding their jobs and families are on the line for speaking their minds, what is happening to that nominal Catholic Enda Kenny? You know the man who closed Ireland’s embassy in the Holy See, who misled the Irish public with regards to the Cloyne Report, pointing the finger solely at the Vatican in a speech loaded with venom and vitriol?
What’s happening to the man who is trying to force priests to legally be compelled to break the seal of confession? Ah yes, that’s right a Catholic University is awarding him an honorary doctorate.
“Prime Minister Kenny is an internationally respected leader with a well-known reputation for promoting human rights and causes of social justice, two issues that resonate with the Boston College community,” said University Spokesman Jack Dunn.
Only if you are born it would seem.
This is the man who pitched up at Knock international airport to unveil a statue of a Catholic Monsignor (Knock being a noted site of holy pilgrimage) on a weekend that saw an influx of Catholic pilgrims praying for the unborn, and responded to threats of excommunication saying ‘I have my own way of speaking to God’.
What in the name of all that’s holy, is this all about? What a kick in the teeth. Disgusted, scandalized, demoralized, doesn’t begin to cover it. Demonic comes somewhere close perhaps.
Yesterday on Twitter saw a Catholic GP being forced to close down his Twitter account following an episode of online bullying which resulted in his being reported to the NHS as well as the GMC, for the heinous crime of referring to the number of abortions in the UK as ‘the slaughter of babies’.
I witnessed the whole incident, having previously blocked those responsible – there is a posse of Irish pro-abortion advocates on Twitter, who swoop on every single Tweeter who dares to express an opinion upon the current state of affairs in Ireland. Over the past few weeks every single time I have said anything about abortion and Ireland in the same 140 characters, a persistent gang has appeared from out of the blue to attack with insult and invective. Yesterday’s ‘debate’ saw them swooping in with the same discredited narrative regarding the death of Savita Halappanavar, and then going on to attack me, a non Irish national for daring to defend the rights of the unborn in another country.
There’s nothing more of a disincentive in terms of engaging on Twitter to scroll down one’s mentions column and see numerous rants on the same subject, by the same few determined people, chock full of angry and impassioned hypberbole, together with personal insult. Besides which those who seek to discredit an international symposium of gynaecologists as being ‘liars’ on the basis that one disagrees with their conclusions and who decry Ireland’s outstanding maternal death rates as being ‘lies’, don’t really incline one to do anything other than block. One should note, nonetheless, that these are the same people who repeatedly attacked those who they deemed to be not medically qualified and therefore unable to comment, but who repeatedly seized on the subjective opinion of openly pro-choice expert Dr Boylan as being definitive medical fact in the Savita inquest, despite the fact that 11 other experts publicly disassociated themselves from his stance. Clearly they were obviously lying too.
I tweeted a few responses, realised this was a futile exchange, hit the block button repeatedly, switched off the phone and trundled off to the park with the children to make the most of the Bank Holiday sunshine. Yet another day, yet another Twitter spat?
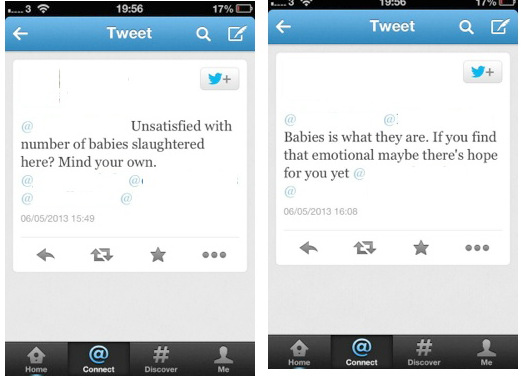
Not quite. Later on that evening I discovered that one of my followers, a Catholic GP had joined in the fray, referring to UK interest in the Ireland abortion debate, as having seen almost 200,000 babies slaughtered here on an annual basis and not wanting Ireland to go down the same route. Here’s what he said.
The pro-aborts took issue with the fact he had referred to unborn children as babies and went for the jugular, causing him some considerable concern. (Apologies for the blurry images, I’ve deliberately obscured identities).
The pro-aborts reported him both to his employers at the NHS and the GMC, because they determined that referring to the unborn as ‘babies’ and by the almost 200,000 abortions that occur in the UK on an annual basis, he was in fact taunting women who had abortions as being ‘baby slaughterers’, and there was thus legitimate cause for concern that he could be taunting women patients.
What these so-called advocates of science and reason could not cope with was the presence of a medic, undermining their rhetoric about the unborn, hence they threw their toys out of the pram and decided to put his job in jeopardy or at least attempt to. On seeing that he had deleted his account, one therefore relented slightly and said that she had withdrawn all her tweets to the NHS. How very generous.
Job done. Serves him right. Hopefully he’ll think twice about expressing the fact that as a doctor he opposes abortion in public ever again. That’s another one closed down. These people need to be an example of.
Of course let’s remember that at least two of these tweeters were those who had expressed apoplexy that a UK tweeter might engage with the political situation in Ireland, yet had no compunction reporting an UK doctor to his professional body on the basis of a firmly expressed view, which was by the way, perfectly in accordance with the GMC guidelines on how medics should use social media. These guidelines specifically encourage doctors to take part in public health and policy decisions as well saying that doctors should identify themselves.
All of which went above the heads of the pro-aborts who said that he was fair game. He had no right expressing his own opinion, which was clearly religiously based.
But all of this was his own fault.
Another Tweeter joined in the fray to defend said GP. So enraged were these advocates that someone else dared to disagree with them, that they then felt compelled to hunt down this interlocutor, believing it to be the GP’s wife. I mean. How dare she go on Twitter to defend her husband who is having his professional competence and employment threatened on the basis of expressing a point of view and for stating that he was a Catholic GP in his bio. Oh the audacity, let’s find out all about her too, shall we. Let’s track down her Facebook profile.
At which point I begin to call out their behaviour.
Because this sort of probing into one’s family life and personal details is the behaviour of a reasonable and rational person.
Ben has written about this and it would seem he is right. Catholics need to be increasingly prepared to defend themselves from these sort of threats and attacks if they expound their views on a public forum and particularly if they are perceived to be in a position of influence.
These people are unrepentant this morning, claiming that this GP deserved to be reported for taunting women as being ‘baby slaughterers’ and telling others, such as @battlementclare that they would not hesitate to report her too, if she were still a practicing midwife, or indeed anyone who was involved in medicine and vocalised pro-life views.
I don’t generally like to go down the whole ‘persecuted Christians’ schtick. But not once in this entire debate, did either myself or the GP allude to God, yet it was the pro-aborts who kept bringing Him into the discussion as being a reason why we must not be taken seriously or listened to. Our arguments were wholly secular, though both of us are openly Catholic and proud to profess ourselves as such.
Losing one’s job may not seem to be in the same league as being thrown to the lions or physically tortured, beaten and killed as a result of one’s beliefs and faith. But being disbarred from a particular profession unless one agrees never ever to voice one’s own views, being sacked and unable to support one’s family, being ostracised and having one’s family targeted as a result, brings us a step closer.
Let us hope that the GP and his family take comfort from the recent words of Pope Francis. They need our prayers.
“[The apostles’] faith was based on so powerful and personal an experience of Christ crucified and risen, that they were not afraid of anything or anyone, and even saw their persecution as a badge of honor, that made them capable of following in the footsteps of Jesus and to be like Him, bearing witness with their lives,”
“… and in these times, there are many Christians who suffer persecution, a great many, in many countries: let us pray for them from our heart, with love, that they might feel the living and comforting presence of the Risen Lord.”
Cardinal Dolan’s officials refused entry into St Patrick’s Cathedral, New York to a group of LGBT protestors who had deliberately dirtied their hands in protest at a recent blogpost of his, in which he shared an anecdote from his childhood to do with his delight when his best friend was allowed to join them for dinner, but was told that first he would need to wash his hands:
I was so proud and happy. Freddie was welcome in our house, at our table. We both rushed in and sat down.
“Freddie, glad you’re here,” dad remarked, “but . . . looks like you and Tim better go wash your hands before you eat.”
Simple enough . . . common sense . . . you are a most welcome and respected member now of our table, our household, dad was saying, but, there are a few very natural expectations this family has. Like, wash your hands!…
So it is with the supernatural family we call the Church:all are welcome!
But, welcome to what? To a community that will love and respect you, but which has rather clear expectations defining it, revealed by God in the Bible, through His Son, Jesus, instilled in the human heart, and taught by His Church.
Surely the point is clear enough? Everybody is welcome, rich, poor, young, old, black, white, gay, straight, married, single, but the Church has the same expectations of everyone regardless. One couldn’t ask for a greater definition of equality.
But no, in an overblown statement of victim rhetoric, Joseph Amodeo writing for the Huffington Post says, that the Cathedral is his home from which he has now been evicted and that now he is spiritually homeless. In colourful prose, he describes the ‘cold hard steel and the means by which the doors closed’ (what on earth does he mean by that, I’d never thought of door hinges as being particularly loaded with menacing metaphor and if he’s referring to the doors needing to be pushed shut, isn’t that exactly how they were designed?) capturing the sentiment that they were not welcome.
Actually all of the activists were more than welcome, but were requested to wash their hands first. Quite right. In a Mass, especially if one receives communion, we encounter Christ. Why would anyone deliberately make themselves filthy to meet their King and Redeemer. It’s a deliberate act of blasphemy. Whilst it makes for another good argument for receiving communion on the tongue, making oneself dirty in order to use a church to make a political protest is highly offensive. And what about shaking hands during the sign of peace? Would they have deliberately and ostentatiously rubbed their mucky paws and transferred grime onto other peoples’ hands who might be receiving communion. Even had they exercised courtesy and respect to fellow Mass-goers it still makes a mockery of the Holy Spirit, restricting sharing the peace with a small select clique.
A protest of this type has no place within a religious setting. I’d like to see them attempt to enter a mosque with their shoes still on. Like Lisa Graas, I cannot get my head around anyone who would intentionally make themselves dirty before receiving Christ in the Eucharist. Christ loves us and meets us where we are, but as Cardinal Dolan says, this encounter always involves a recognition on our part that we need to clean up first. The Eucharist is a meal, of course we should make every effort to be spotless, internally and externally before receiving of the body of Christ.
This protest or ‘silent witness’ subverted the Christian message to being about love of self. The Lord loves us in spite of our dirt and filth, He can certainly see beyond it, but that doesn’t preclude us trying to rid ourselves of it. Dirt or sin, matters, it keeps us from having the close relationship which we need. Whilst Christ welcomed the poor, the outcast, the dispossessed, he touched those who were deemed unclean, none of those who came before him had deliberately put themselves in this state in the first place and certainly none were celebrating it and demanding that they should be healed, or that it was their right.
Filth is no barrier to encountering Christ. It makes it all the harder when we deliberately wallow in and celebrate it nonetheless. My children are prone to some absolutely physically disgusting behaviour. When one of my daughters comes to me covered in sticky chocolate, sudacreme, liquid soap, caked in mud or worse, I’ll still love them as fiercely as before, but will literally hold them at arm’s length until I’ve dumped them in the bath. I don’t pander to temper tantrums about not wanting to clean up and being fine as they are. Particularly, when like the organiser of this vigil, they have a history of throwing their toys out of the pram and hurting other people when they don’t get their own way.
Christ always extends a welcome. But on His terms, not ours.
I hate to sound like a conspiracy theorist, but I am becoming increasingly unnerved by the clamour being made by those in the business of sex education, such as assembled ‘experts’ who are repeatedly calling for better state sex education in schools, including teaching pupils that ‘not all porn is bad’.
No doubt these are the same advocates who bitterly complain about the ‘indoctrination’ of pupils in faith school, who seem to be utterly blind to the irony that even espousing a so-called neutral view, is an ideology in and of itself. I am boggling at how the notion ‘not all porn is bad’ can be seen as anything other than subjective opinion.
As for becoming porn literate (and I cannot bear that particular neologism), what does that really mean? As in the sense of computer literate, i.e. having competence or knowledge? Or more likely, being able to think critically about porn, able to discern between what is good and what is bad? And who on earth makes those decisions? What constitutes good or bad pornography or erotica is entirely dependent upon the subjective lens of the recipient and their personal tastes. Not to mention Aristotle, under whose definition all pornography is good. Those who complain vociferously about the role of the nanny state when any changes to the law regarding the accessing of internet porn are mooted, ought to think about long and hard about whether or not our children should be taught that xyz makes for ‘bad’ porn, whereas something else is deemed as ‘good’ as well as the acceptable context in which to use porn.
And let’s face it, in order for children to be taught how to become discerning viewers of porn, they are going to need to be exposed to a fair few different genres and the whole point of porn is that it is not designed to be rational. Responses to pornography are never rational or cerebral they are always visceral, instantaneous and physical which is why it is so hugely popular and addictive. Habitual users of porn are well aware that rationally and intellectually, it isn’t realistic, addicts are often well aware that a porn addiction is psychologically unhealthy and impede real-life relationships, but it’s never that easy to wean oneself off, especially when the next hit is only a click away. And let’s not kid ourselves about the purpose of porn either. It really isn’t rocket-science to note that the release of the various neuro-chemicals and hormones involved in reaching climax are an intoxicating and heady mix, as this secular site, designed to help young men beat a pornography addiction, explains. Whilst there are several other Catholic resources designed to help people spiritually, such as for example porn no more, reading about the science behind the effects of porn upon the brain, is both compelling and terrifying.
Exposing children to porn, even with good intentions, borders on the abusive. It normalises and contextualises something that should be a taboo, as being a perfectly harmless habit. Thirty years ago, if men wanted to see porn, it would involve a fair bit of effort, such as shuffling off to the newsagent when no-one else was around or attending a grubby and squalid peep show in the backstreets of Soho. The internet enabled burgeoning of the porn industry has been every male pervert’s dream, no longer are they seen as sordid, seedy, sleazeballs but as sophisticated consumers of a product. And women have been co-opted in their own sexual objectification to a degree that would have been unthinkable just a generation ago.
Children, especially teenagers faced with fluctuating levels of hormones, are not intellectually equipped to make decisions about sex, whilst not lacking intelligence, they lack the requisite wisdom that comes with experience. Exposure to porn at this age is especially harmful, whetting their appetites and forming neural pathways and associations with pleasure that will inevitably require rewiring. Most men of my generation admit that their first exposure to porn was via some mucky magazines found in their father’s bedroom or study, or surreptitiously sneaked into school. They also admit that these early experiences seem to have shaped various ideas and preferences, again, one doesn’t need to be an expert on Freud or psychology to understand that early feelings of sexual arousal and the accompanying associations, can prove enormously powerful. It’s stupefying naivety and ignorance to believe that by discussing and attempting to rationalise pornography with children, that they will then be able to control their physical responses to it. It could well backfire in that by deeming certain porn ‘bad’ it becomes ever more alluring.
A school classroom made up of thirty pupils of differing stages of sexual and emotional development is not the appropriate place for discussions of this nature. The schoolteacher is not responsible for the sexual formation of a young adult.
Which is also why the classroom is not the place to teach about what the state regards as ‘good relationships’. Why does the state believe that it has the monopoly on defining and teaching about such deeply personal matters. Most of us are able to recognise an innately dysfunctional relationship, even if we were brought up in such an environment ourselves. Whilst we might need help in identifying and overcoming issues that may have occurred as a result, even those in abusive relationships realise on one level that what is happening is not the ideal state of affairs. There are many complex factors that are involved in why people may end up in abusive relationships, that they were not taught how to recognise them at school seems to be an insignificant factor, generally people find themselves trapped for a variety of reasons, relationships that turn toxic, usually do so gradually.
As for teaching primary school children about adult sexual relationships, instead of ‘placing too much emphasis on friendships’, speaking as a parent of a 9 year old who will soon approach puberty, this is unbelievable stuff. A child’s world is made up of their friendships, when something goes wrong in the playground it can have devastating consequences. Of course the emphasis must be on friendships and how to get along with others, how to be kind, generous and respectful. Priming children as to what healthy adult sexual relationships should look like, is akin to grooming and leaves them very vulnerable to predatory adults.
Whilst of course, any PSHE element should help children to recognise and ask for help in terms of unwanted sexual behaviours or advances, there is a danger in placing emphasis upon a good quality sexual relationship, almost as if this should be a given in a romantic relationship or is indeed a necessary part of a fulfilling life. By teaching children a subjective definition of good and bad relationships, they also encourage a tendency to discard anything that falls short of the ideal standard, or when things become difficult, when very often problems and difficulties can be rectified.
Relationships are not always ideal and perfect, from the Catholic point of view we know that the graces conferred upon us by the sacrament will reinforce us, but ultimately even the best marriages go through the odd sticky stage. Which is why the marriage vows include a promise to love, which sometimes requires an act of will, it is not simply a confirmation of being romantically in love, but a promise to love the other person, even when they are being at their worst.
What seems apparent is that the state is trying to package up, homogenise and clinicalise every single sexual relationship and impose this utopian vision upon our children. This is the type of sex you should be having, here’s the type of relationship that you should have and here’s the pornography that is okay to look at and here’s how you should use it. It feels deeply unpleasant and intrusive.
I read earlier that the pornography industry is becoming safer than the food industry when it comes to health and safety standards. Which really says it all. Do we really want our sexual relationships monitored, regulated and served up to us like a tasteless, plastic, microwave meal. Or do we want something home-made, free of artificial ingredients, wholesome, comforting, heart-warming, authentic, nutritious and made with human love and care. It might not look as perfect or uniform as the mass produced product you take out of the packet, or be made conforming to the same stringent standards of health and safety. It may often be harder to produce. But it sure tastes and feels infinitely better.
Do we really want children sold a state-sanctioned convenience-meal version of sex and relationships?
Last week I received an awful lot of flack on Twitter and in other places, for my writing on the case of Savita Halapannavar. The main criticisms seemed to be that being neither Irish nor a qualified medic, I had no right or authority upon which to pass comment.
Every single medical fact I commented upon was not made without reference to highly experienced qualified doctors and midwives, all of whom were in disagreement with Dr Boylan, whose testimony that a termination would almost certainly have saved Savita’s life, was widely quoted by the pro-abort activists as being proof that the law needed to change, as it was, in his opinion, responsible for her death.
The reason that this case has needed to be scrutinised in intricate detail, is because it was so quickly seized upon by those championing abortion in Ireland, as being definitive proof that lack of abortion was leading to unnecessary deaths. What I am more than qualified to state, is that abortion devastates lives and causes infinite pain and hurt to many women, (and men) as well as ending the lives of their babies. By all accounts Savita was a lively caring, compassionate woman. The last thing she would have wanted was for more pregnant women to be vulnerable as a result of her death.
I have just received a copy of the following press release from John McGuirk which I have replicated in full.
Ends
Dear Sir:
The recent inquest on Ms Savita Halappanavar has raised important issues about hospital infection in obstetrics. Much of the public attention appears to have been directed at the expert opinion of Dr Peter Boylan who suggested that Irish law prevented necessary treatment to save Ms Halappanavar’s life. We would suggest that that this is a personal view, not an expert one.
Furthermore, it is impossible for Dr. Boylan, or for any doctor, to predict with certainty the clinical course and outcome in the case of Savita Halappanavar where sepsis arose from the virulent and multi drug-resistant organism, E.coli ESBL.
What we can say with certainty is that where ruptured membranes are accompanied by any clinical or bio-chemical marker of infection, Irish obstetricians understand that they can intervene with early delivery of the baby if necessary. Unfortunately, the inquest shows that in Galway University Hospital the diagnosis of chorioamnionitis was delayed and relevant information was not noted and acted upon.
The facts as produced at the inquest show this tragic case to be primarily about the management of sepsis, and Dr Boylan’s opinion on the effect of Irish law did not appear to be shared by the Coroner, or the jury, of the Inquest.
Obstetric sepsis is unfortunately on the increase and is now the leading cause of maternal death reported in the UK Confidential Enquiry into Maternal Deaths. Additionally there are many well-documented fatalities from sepsis in women following termination of pregnancy. To concentrate on the legal position regarding abortion in the light of such a case as that in Galway does not assist our services to pregnant women.
It is clear that maternal mortality in developed countries is rising, in the USA, Canada, Britain, Denmark, Netherlands and other European countries. The last Confidential Enquiry in Britain (which now includes Ireland) recommended a “return to basics” and stated that many maternal deaths are related to failure to observe simple clinical signs such as fever, headache and changes in pulse rate and blood pressure. Many of the failings highlighted in Galway have been described before in these and other reports.
The additional problem of multi-resistant organisms causing infection, largely as a result of antibiotic use and abuse, is a serious cause of concern and may lead to higher death rates in all areas of medicine.
Ireland’s maternal health record is one of the best in the world in terms of our low rate of maternal death (including Galway hospital). The case in Galway was one of the worst cases of sepsis ever experienced in that hospital, and the diagnosis of ESBL septicaemia was almost unprecedented amongst Irish maternity units.
It is important that all obstetrical units in Ireland reflect on the findings of the events in Galway and learn how to improve care for pregnant women. To reduce it to a polemical argument about abortion may lead to more – not fewer – deaths in the future.
Yours sincerely,
Dr. John Monaghan, DCH FRCPI FRCOG Consultant Obstetrician/Gynecologist
Dr. Cyril Thornton, MB BCh MRCOG Consultant Obstetrician/Gynecologist
Dr. Eamon Mc Guinness, MB BCh MRCOG Consultant Obstetrician/Gynecologist
Dr. Trevor Hayes, MB BCh FRCS MRCOG Consultant Obstetrician/Gynecologist
Dr. Chris King, MB DCH MRCOG Consultant Obstetrician/Gynecologist
Dr. Eileen Reilly, MB ChB MRCOG Consultant Obstetrician/Gynecologist
Prof John Bonnar, MD FRCPI FRCOG Professor Emeritus Obstetrics & Gynaecology
Prof Eamon O’Dwyer, MB MAO LLB FRCPI FRCOG Professor Emeritus Obstetrics & Gynaecology
Prof Stephen Cusack, MB BCh FRCSI Consultant in Emergency Medicine
Dr. Rory Page, MB BCh FFA RCSI Consultant Anaesthetist
Dr. James Clair, MB BCh PhD FRCPath Consultant Microbiologist
I know we should no longer be surprised when it comes to politicians displaying a capacity to lie to and deceive the general public, but the behaviour of two Irish Labour TDs, Aodhan O’Riordain and Anne Ferris really takes the cake.
Today’s Irish Sunday Independent (colloquially known as the Sindo) has run an exclusive splash, revealing that last June, four months before the death of Savita Halappanavar, these two politicians were caught on tape, explicitly outlining their intentions to use the X Case, (where suicide is deemed to be a life-threatening condition and thus a reason to abort) as a ‘starting point’ to introduce liberal abortion laws into the country.
Regardless of whether one takes a pro-life or pro-choice stance, this disingenuous approach is to be condemned. Politicians are elected on the basis that they represent those who vote for them. Aodhan O’Riordian stated that the X Case was a ‘starting point’, however if he were to be asked that question on the radio, his approach would be to lie about it, denying that it was a starting point and stating that ‘it is what it is’.
“It is a starting point. Once you get that . . . then you can move . . . and of course if I’m on the radio and somebody says to me, ‘It’s a starting point for abortion on demand’, I’m gonna say, ‘No, of course it isn’t – it is what it is.'”
Anne Ferris said
We will legislate certainly for what the European Court has told us to and then we can go further than that . . . we get the first part done and then we will go on to the next bit… I would say then next term it will happen.”
The transcript of the conversation also shows Ferris promising to drink a bottle of champagne after this measure is passed. This matters, not simply because of the subject matter, but also because it is a case of blaring political hypocrisy, whereby elected politicians are once again making monkeys of the electorate, lying about their stated intent and who will no doubt later agonise over the general public’s disillusionment with politicians and voter apathy.
Lying is never acceptable, but one’s intentions with regards to abortion, (or reproductive rights if you’re on the other side of the debate) is far too important an issue to lie about to the public. The attitude on display here is nothing short of contemptuous.
When it comes to thinking about the X Case and whether abortion ought to be a remedy for those who may be suicidal, it’s worth remembering that in the case of a person who may be suicidal, this is almost always due to a perfect storm of contributing factors, of which a setback such as a crisis pregnancy provides the tipping point. People who are suicidal or who suffer from severe mental health issues are deemed to be (albeit temporarily) incapable of informed consent in law, wills and other legal contracts are deemed to be invalid, so why, all of a sudden is a threatened suicide deemed to be a valid reason to abort one’s unborn child?
There is no evidence to suggest that abortion is an effective therapy for a psychiatric problem, which needs to be solved by psychiatric means, but there is an substantial body of research suggesting that abortion has a negative impact upon mental health. Suicidal tendencies in themselves should not be confused with a medically life-threatening condition. Whilst suicide is of course life threatening, the desire to end one’s life, is not indicative that a person will necessarily follow through on their thoughts, though they do of course, require urgent help. Abortion circumnavigates the issue, confirms the woman in her despair and is not indicative of the most compassionate and caring approach. What if the woman caught up in the vortex of depression, aborts her baby and later bitterly regrets her decision, realising that her fears about her pregnancy or ability to mother her child were unfounded?
David Fergusson, a pro-choice doctor, who believes that abortion should be available on social or economic grounds, has published a peer-reviewed study in this month’s Australian and New Zealand Journal of Psychiatry, in which he reviewed the research to ascertain whether or not there were any mental health benefits to abortion. His findings were clear, as Breda O’Brien, is at pains to point out in the Irish Times:
“at the present time there is no credible scientific evidence demonstrating that abortion has mental health benefits.
The evidence will
“resurrect politically uncomfortable and socially divisive debates”. “However, it is our view that the growing evidence suggesting that abortion does not have therapeutic benefits cannot be ignored indefinitely, and it is unacceptable for clinicians to authorise large numbers of abortions on grounds for which there is, currently, no scientific evidence.”
With blatant disregard for scientific evidence as well as the views of the Irish electorate as a whole, a sizeable majority of whom wish to keep Ireland’s current laws protecting the unborn, the Irish Labour party are wishing to push and impose their ideological agenda on an unwilling public. It’s also interesting to note that 66% of voters are concerned about the EU’s potential to intervene in Irish pro-life laws.
As things currently stand, the Irish Supreme Court would be unable to accept any laws or proposals that go further than legislation on the X case, this being against the Eighth Amendment of the Constitution which reads as follows:
The State acknowledges the right to life of the unborn and, with due regard to the equal right to life of the mother, guarantees in its laws to respect, and, as far as practicable, by its laws to defend and vindicate that right.
Any legislation beyond X (and that’s accepting that suicidal people should be able to kill their unborn children to make them feel better) would require a repeal of the Eighth Amendment and a rejection of personhood.
All of which could spell trouble for Ireland’s coalition government led by Enda Kenny, leader of Fine Gael, with Labour’s Eamon Gilmore occupying the Deputy Prime Minister position. Fine Gael explicitly promised voters in 2011 that they would not legislate for abortion and over 40,000 voters have signed a pledge never again to vote for the party if they introduce abortion measures. Worryingly for Enda Kenny, John Bruton, a former Fine Gael leader and Taoiseach is one of those also publicly opposing the coalition’s abortion proposals as are several members of the Fine Gael party. What is telling is that if Ms Ferris is to be believed, the tail is very much wagging the dog, when it comes to Ireland’s coalition government, with Eamon Gilmour, apparently ordering Enda Kenny to whip Fine Gael TDs into line on the issue of abortion. Extraordinary stuff, it’s a bit like Nick Clegg trying to tell David Cameron to whip Tory MPs into line with Lib Dem thinking.
This weekend in the UK has seen the forty-fifth anniversary of the passing of the 1967 Abortion Act, which was sold to the British public on the grounds of compassion and helping women from dying in desperate circumstances. We now see over 200,000 abortions a year, more than 1 in 4 pregnancies are aborted and the numbers of those aborting under grounds F or G (to save the life of the pregnant women or to prevent grave permanent injury) are, in the words of the Department of Health, ‘exceptionally rare’. Grounds A and B that pertain to the risk of death or permanent injury of the pregnant woman account for a tenth of 1% of all abortions.
And yet, Ireland’s politicians perpetuate the myth that this is a necessary piece of legislation in order to further their own totalitarian ideology when it comes to the rights of the unborn. It’s a baffling state of affairs and one in which pro-lifers must do their best to support Ireland, whether that be via prayers or practical action. Ireland is a model of maternal care. It is the gold standard and a torch bearer for Western democracies everywhere. Ireland’s pro-life movement is cohesive, cross-party and pan-theistic, able to mobile huge numbers of people onto the streets to vocalise their support for the unborn. There are many lessons there for the UK, but equally Ireland must look to the UK as an example of how not to do things.
These revelations could be a crucial pivot in Ireland’s battle for life. What an own goal for Irish Labour and those advocating for Action on X.
Before going any further, we should all remember Savita’s husband Parveen Halappanavar in our thoughts and prayers. Today, the date that the inquest returned its verdict of medical misadventure following the death of his wife, they should have been celebrating their fifth wedding anniversary together with their newborn baby girl due to be be named Prasa. May they rest in peace.
There are already many disingenuous headlines in the press, stating that the inquest has ruled medical mismanagement, following the denial of an abortion to Savita, as if the two events are linked.
First of all, Savita was not denied an abortion, rather a termination of pregnancy. Though it may seem semantic, this is an important distinction. Though medically they both refer to the same end result, the term abortion is widely understood in the context of a woman who does not wish to have a baby. With women such as Savita, a termination of pregnancy is the more correct phrase, because the pregnancy and baby were accepted and welcomed. Savita wished for her pregnancy to be terminated swiftly when it became clear that she was miscarrying. She didn’t want to abort her unborn child, she wanted her miscarriage to be brought to a quick conclusion.
Savita’s request for her pregnancy to be terminated must be seen in the context of her miscarriage. The explanation given at the inquest, that this was not carried out because of the law, is an unsatisfactory one. The implication being that though there was a good medical reason to terminate the pregnancy, the law disallowed this.
Dr Katherine Astbury testified that on the Monday and the Tuesday, Savita did not appear to be unwell, though she was emotionally distressed. In these circumstances, Dr Astbury is quite correct, Irish law would not allow for a termination to take place, because there appeared to be no risk to Savita’s life. This is actually fairly reasonable. Poor prognosis for the foetus would not allow for a termination, because Ireland rightly places equal value on all life, born and unborn alike. That someone has a poor prognosis is not grounds to kill them. Patients who are given a diagnosis of a terminal or incurable disease are not then killed because the outlook looks bleak and neither are the elderly, much as people might agitate for euthanasia. Whilst there is life, there is always hope and when we take into account the fact that Savita’s pregnancy was a wanted one, so long as a life is not deemed to be at risk, then it is not morally acceptable to kill an unborn baby on the grounds that he or she is as likely going to die soon anyway.
The request to terminate the pregnancy from Savita, should not have determined what was in her best medical interests. All other things being equal, normal medical protocols dictate a conservative management (i.e. wait and see) approach. On a personal note, I can well imagine her distress and her physical pain. I was readmitted into hospital a week after my eldest child was born, suffering from retained infected placenta. When I apologised to the registrar in A&E for crying because I was in so much pain, his response was ‘madam, you have a uterine infection, it is going to hurt a lot’. In my case, despite my entreaties, they didn’t take me in for surgery for 4 days (it was Easter bank holiday weekend) preferring instead to administer IV antibiotics to cure the infection first and to see if the product would pass. Nine years on, I can still remember the pain vividly, but at least I was given the correct antibiotic treatment, though my desire to have a D&C and be back home was ignored. I can’t begin to imagine what Savita went through, especially when she had the ultrasound and could hear the heartbeat of her baby, whom she knew was shortly to die. It must have been awful for her and her husband, let’s not forget that.
But this question of abortion or termination is nonetheless the source of much misinformation. Speaking at the inquest Dr Astbury stated that had she known about Savita’s blood results on Monday or Tuesday, then she would have taken a different decision and terminated Savita’s pregnancy forthwith. Which begs the obvious question, why didn’t she? We know from the inquest that the blood test results taken from Savita at 6.33pm on the Sunday evening were immediately processed and were available on the hospital’s computer system at 6.37pm. They were not accessed until 5.24pm the next day, by an unidentified member of staff and Dr Astbury herself did not look at them until 11.24pm on the Wednesday morning, by which time Savita’s condition had severely deteriorated.
It is this delay that proved fatal for Savita. If a termination had been required, then Irish law allowed for this, the medical guidelines state that delivery of an unviable foetus may be expedited where there is real and substantial risk to the life of the woman. Sepsis would count as such a risk. Savita’s bloodcount was 16.9 (normal range 4.3 – 10.8) which should have rang alarm bells. She was definitely exhibiting signs of an infection which merited urgent further investigation which would have thrown up the presence of E.Coli. Real and substantial risk, are often confused with immediate. A woman does not have be in her death throes or dying for a real and substantial risk to be identified, simply that if a termination is not performed, there is a real and substantial risk that she will die.
With hindsight, this perhaps was the case with Savita, as she was at risk of chorioamnionitis (inflammation of the foetal membranes), once the membranes had broken on Sunday. Once this has happened there is a 30 – 40% risk of infection, which is why she was prescribed general oral antibiotics on the Monday evening. Had Dr Astbury thought Savita was at risk of this, or was exhibiting signs, then why were no further diagnostic tests peformed, in this case an amniocentesis would have confirmed whether or not chorioamnionitis was present. Regular monitoring to identify trends in the white blood cells count is also crucial.
What has confused the issue further is that Dr Peter Boylan, a doctor with a publicly stated position opposing abortion restrictions, testified as an expert witness stating that had Savita been allowed a termination earlier, it would have saved her life. It’s very difficult to know that with any certainty without recourse to a time machine. In any event the post mortem showed that it was the E.Coli bacteria that led to septic shock. The baby was not poisoning Savita’s bloodstream, though chorioamnionitis if diagnosed, requires delivery. If the baby had died then the placenta needed to be removed in order to halt the rapid of spread of infection spread via its dead blood cells. Bacterial chorio-amnionitis is exceedingly rare.
What we do know though, is that in 40 years there have been 5 cases of septic abortions, no patients have died and Savita’s case was very rare. Every year in Ireland there are sadly 14,000 miscarriages, many of them carrying an infection risk, and no maternal deaths on record where the obstetrician felt that the law was inhibiting them. Dr Sam Coulter Smith, master of the Rotunda Hospital in Dublin, says that he has terminated a pregnancy in four instances where women had been diagnosed with sepsis and in all of them the baby did not survive. It’s difficult to see then, how Irish law can be said to be putting women at risk.
The failure of Dr Astbury to discuss abortion outside of legal terms is what has proved troubling in this case. A surgical abortion would have carried with it real risks of further infection which could have proved fatal, and had Savita been given the drug misoprostel to induce delivery, this would not necessarily have made delivery any swifter or negated the need for surgical intervention. Faced with a fully dilated cervix and ruptured membranes, the medics could thought that delivery was imminent and there was therefore no need for further medical intervention at this point. They were therefore wholly wrong not to discuss this in medical terms with Savita and her her husband. Anyone would be cross if their request for a certain type of medical treatment was refused purely on legal grounds.
What is important is that today’s inquest ruled that there was medical mismanagement in the death of Savita Halappanavar. The jury had the option to deliver an a narrative verdict which would not have attributed a cause. Despite the verdict which implies failures in medical care, the judge, Dr McLoughlin, has thrown further confusion into the mix by stating the verdict did not mean that deficiencies or systems failures in University Hospital Galway contributed to Ms Halappanavar’s death; these were just findings in relation to the management of her care.
That seems to imply that there was nothing wrong with the general systems in place at University Hospital Galway, simply that the management of Savita’s individual care was unsatisfactory as we can see. One cannot help but wonder whether or not this is about offloading any legal liability that the hospital may incur in terms of compensation that might be due? After all, it was a galloping sepsis that killed Savita, stemming from the E.coli, ESBL bacteria that entered her bloodstream from the urinary tract and one that is antibiotic resistant. No-one can say with any certainty whether, even had the care been perfect, she would have survived this. Perhaps that is what the coroner is trying to convey, medical misadventure was a factor in relation to her care, but not necessarily in her death. It’s no wonder Parveen is still in the dark.
What urgently needs to be addressed is the factors behind the poor care. Did the law really make Dr Astbury too afraid to check blood results, which needed further analysis or carry out further diagnostic tests? Was the law behind the lack of regular observations, the lack of communication and the failure to realise that paracetamol administered as a painkiller could mask other symptoms? Did the law cause staff to forget that infection requires a low burden of proof? Or was it the effects of austerity measures on an already overstretched hospital struggling with lack of resources? What caused the glaring omissions and can any law be expected to cover every single permutation that might arise in the management of pregnancy or childbirth, or is this simply that medical guidelines need to be more precise and explicit?
Here is the list of the coroner’s recommendations which the jury all unanimously and strongly endorsed
* The Medical Council should say exactly when a doctor can intervene to save the life of a mother, which will remove doubt or fear from the doctor and also reassure the public;
* Blood samples are properly followed up;
* Protocol in the management of sepsis and guidelines introduced for all medical personal;
* Proper communication between staff with dedicated handover set aside on change of shift;
* Protocol for dealing with sepsis to be written by microbiology departments;
* Modified early warning score charts to be adopted by all staff;
* Early and effective communication with patients and their relatives when they are being cared for in hospital to ensure treatment plan is understood;
* Medical notes and nursing notes to be kept separately;
* No additions or amendments to be made to the medical notes of the dead person who is the subject of an inquiry.
Savita’s request for a termination to have been accepted and acted upon, simply by dint of her wishes. would have required Ireland to have legislation which is much more liberal than even that in the UK, which in practice, allows abortion on demand.
It’s no wonder that the clamours for a repeal of the Eight Amendment of the Irish Constitution, (which defends the right to life of the unborn) have already started. None of which addresses the reasons behind the catastrophic failures in care.
One thing that should be emphasised is how rare it is to have a miscarriage at 17 weeks. 0.5% of single pregnancies in women with no history of recurrent miscarriages end in spontaneous second trimester foetal loss. Sepsis is still thankfully rare. Whilst it should be on the radar as a possibility, most maternity staff will not be panicking about the possibility of sepsis when a pregnant woman presents with a UTI. In the incidence of a UTI, blood samples are tested and antibiotics administered. A normal reaction to a UTI would not be to terminate the pregnancy as a precautionary measure. UTIs are serious if left untreated but no medical protocols would consider them as a real and substantial risk to life. Even with a suspected UTI there was no reason (in the absence of blood results) for medical staff to believe that Savita was dying.
I would be seriously concerned if any medic proposed termination of pregnancy as being necessary as a precautionary measure, unless it was in the most serious and grave of circumstances. Nowhere in NICE guidelines is termination mentioned as a treatment for a bacterial infection. Savita’s death should not prompt pregnant women diagnosed with a UTI to seek abortion and neither should they worry about contracting sepsis. One thing that should be remembered is the importance of scrupulous personal hygiene in terms of preventing the spread of bacteria such as E.coli.
(Perhaps this is what the Archbishop has in mind?)
Archbishop Vincent Nichols must be feeling quite justified. He gives a homily in which he appears to denounce blogs, saying that people are attracted to them because we love to hear complaints and are attracted to gossip, followed by a sentence saying that they should have no place in the Church, and surprise surprise, the Catholic blogosphere goes apoplectic and complains about it, thereby proving his point quite nicely.
The problem is twofold. Firstly the sentence “They should have no place in the Church” is placed (perhaps deliberately) after the sentence which explains why we are attracted to newspapers and blogs. It therefore creates an ambiguity. Is Archbishop Nichols talking about newspapers and blogs having no place in the Church, or rather gossip and complaints? Or both?
He (Pope Francis) knows that we live in a society in which complaining and gossip is a standard fare. They sell newspapers and attract us to blogs because we love hear complaints and to read gossip.
But Pope Francis is clear: they should have no place in the Church
But actually the excellent homilies from Pope Francis to which the Archbishop refers, makes no mention of newspapers and blogs, he talks about how complaining dashes hope, as well as the evils of gossip.
But is Archbishop Nichols really saying that newspapers and blogs have no place in the Church? I don’t think this can be the case, not least because the Vatican has its own newspaper and blog. It might have been more helpful had he been a little more precise, i.e. newspapers and blogs that are solely devoted to gossip and complaining have no place in the Church, although this too would have aroused ire. The Archbishop in a bit of a no-win situation whatever he says regarding blogs and the internet.
The other problem is in the assertion that people are attracted to newspapers because they are attracted to gossip and like to hear complaints. This assumes ill-will or bad intention on behalf of the reader which is not always present. I don’t read the Catholic Herald, for example, because I want to hear gossip, (not that the Herald publishes any) if I wanted ecclesial or clerical gossip there are much juicier sources, but because I like to read about what’s going on in the Catholic world as a whole and read some informed, educated and orthodox commentary from those whose opinions I might respect. The same goes for the blogs, my favourites being the priest bloggers (Valle Adurne is a particular treat, I love Fr Sean’s gentle perspectives) and the blogs I regularly read which are written by the laity, again are the opinions of those people who I respect and might well be able to add a different perspective or dimension to an issue which I have not thought about, the most recent that comes to mind is Counter-Cultural father’s outstanding posts on abortion. Likewise I don’t think one can accuse Mark Lambert‘s weekly scriptural reflections as being full of complaints or gossip. Many blogs are genuinely a place of spiritual nourishment.
So, I can well see that backs have been put up by this homily, not least because it assumes bad intent on behalf of bloggers and their readership. Frs Ray and Henry both do a good job in explaining the importance of blogs in democratising the Church as well as explaining the difference between good and bad gossip. Gossip tinged with calumny is the food of Satan.
With all that in mind, I am going to say a few words in defence of Archbishop Nichols and it is very telling that I slightly nervous and mindful of doing this. What kind of situation are we in when an orthodox Catholic is concerned by the reaction that she might receive from the blogosphere, when it comes to defending the most senior Catholic in England and trying to act in good faith?
I understand where ++Vincent is coming from, even though I don’t agree with him. Most members of the CBCEW still don’t quite ‘get’ the internet, although it’s heartening to see Bishop Egan tweeting and blogging. I suspect this is partly a generational issue as well as a not inconsiderable workload. The priest bloggers don’t blog every day, they have their flock to attend to and I’ve been watching the pattern of blogging and noticed (yes priest bloggers, I’m stalking you all) that almost all of them tend to blog in the evening, when they can finally snatch a bit of down time. I suspect that many bishops just ‘don’t get it’ and therefore all they hear about the internet is the bad stuff, i.e. the complaints, the grumbling, the ‘somebody must do something’ and it has perhaps unsurprisingly, coloured their judgement, they don’t get the positive benefits.
Plus, whilst the internet does enable voices to be heard and important concerns to be aired, as we’ve seen with the Gosnell case this week, it does also enable keyboard warriers and online zealots. The internet is a big place which has its fair share of ‘characters.’ Whereas twenty years ago folk would write letters in green ink, now we have the internet which needs discernment and filtration. Here’s a helpful piece that illustrates the usefulness (or otherwise) of Twitter for a mainstream journalist, referring to the aftermath of this week’s tragedy in Boston. Most parishes have at least one, really dedicated and loyal parishioner, who has a particular bugbear who regularly gives anyone who will listen a good earbashing about it. The problem is, that by permanently complaining and finding fault, no matter how legitimate the grievance, over time, repeated grumbling loses its impact.
Those bishops who look upon the internet with scepticism, probably equate it with a troublesome parishioner who never stops grumbling and who never has anything good to say, at least to him, only seeing the difficult or troublesome aspect. If any of them look at the comments boxes on some of the major blogs, their suspicions are confirmed, even the Catholic Herald has its share of ranters. Some coms boxes put me in mind of the bar in Mos Eisley from Star Wars. As Obi-Wan says to Luke Skywalker, “You will never find a more wretched hive of scum and villainy. We must be cautious.” It’s fair to say that charity is sometimes lacking.
So look at it from Archbishop Nichol’s point of view. Bloggers seem to be forever telling him how awful he is, what a terrible job he’s doing and speculating over whether or not he will get, or deserves a red hat. No matter how deserved bloggers might think their criticism, the Archbishop is human, as well as our father in God, that kind of thing would seriously cheese me off too, particularly when they are always threatening to complain to Rome or the Nuncio. We all need not to get carried away by a sense of power.
It’s also fair to say that there are certain blogs and bloggers who do seem to revel in gossip, naming no names. This does have the potential to be dangerous and lead people into error. We have to remember that if we are going to publish a rumour, that there are always two sides to every story, there have been occasions when I’ve read stuff and realised it to be utter bunkum, but I’m not in a position to disabuse it, because to do so would entail breaking confidences and be just as bad as the original piece. It is nevertheless frustrating to see rumour, which like all good gossip has a grain of truth in it, propagated like it is Gospel.
Should anyone be in any doubt about the attraction or power of blogs, Robin, like many Anglo-Catholics, both present and former, used to absolutely devour the blogs, especially Damian Thompson’s, at around the time Anglicanorum Coetibus was issued. It drove me absolutely potty, but is a habit which he has long since eschewed. The reason being, was like many in his position, he had no idea what was going on, didn’t actually know that many real-life Catholics or Catholic clergy and wanted some idea of what was happening and what kind of a welcome or reception he might expect from the Catholic Church should he convert, and also just to get a sense of it. Which is why again, bloggers need to be careful, many of us have crossover readers, internecine squabbling (of which I have been guilty) doesn’t create the best of impressions of UK Catholicism or do much to further the Kingdom. What frustrated me about the blog-checking habit was that to me, what bloggers were saying was utterly irrelevant as to where the Lord might be calling, but I can well see that at a time one feels out of control and uncertain about events, sinful nature leads us to try and be masters and controllers of our own destiny.
Ultimately, if we want to be taken seriously as a force (and I’m talking to myself as much as anyone else here) we need to exercise discernment and ensure that our output is always balanced, reasonable, charitable as well as orthodox and not merely a place for discontented rants or to air personal grievances, again something that I’ve learnt over time. Accusations of clericalism go both ways, neither the hierarchy, nor bloggers and the blogging community should consider themselves beyond reproach or untouchable.
We have to ensure that whatever we do on the internet lives out and advances Gospel values. Otherwise, as Pope Francis says, we run the risk of not recognising Christ walking alongside us.
Those who have ventured onto any mothers’ forums will know that the two topics most likely to end in tears, tend to be those surrounding maternal choices, such as breast versus bottle, methods of childbirth and whether or not to vaccinate.
It’s hardly surprising as these are all choices that every parent has to face at some point or another, we are emotionally invested in our side of the debate, we’ve given the matter considerable thought and are convinced that our choices are the right ones, that have been taken in the best interests of our child. Part of the nature of the human condition is that we all too often seek validation in the opinions and actions of other people and are therefore unable to cope when disagreement rears its head. A decision that runs contrary to our own, implicitly undermines our own judgement – what could be more emotive than the question of whether or not we have done the right thing by our children?
Before I go any further, I’ll set my stall out, in order to invite condemnation/approbation on myself as necessary. All of my children have been vaccinated according to the NHS schedule of immunisations.
The issue of whether or not to vaccinate one’s children, is related to that of the pro-life cause. Rubella in pregnant women can cause miscarriage, stillbirth as well as the following birth defects – hearing loss, brain damage, cataracts and heart problems. Measles can prove equally dangerous. Mumps can cause a higher risk of miscarriage. Furthermore the MMR II Vaccine used in the UK was derived and developed from foetal tissue. Whilst the vaccine itself does not contain foetal tissue, we are not unwittingly injecting children with cells from aborted babies, the cell lines used to create the vaccines were derived from two aborted babies. This is, therefore morally problematic. This does not mean that Catholics should not have their children vaccinated, the Pontifical Academy for Life issued a statement to the effect that innocent children must not be put at risk, particularly in the case of a disease such as rubella, and thus vaccines can be used if there is no available alternative, however parents have a moral responsibility to use these where possible and also to continue to put pressure on the pharmaceutical industry. Here is a link to a website containing a list of which vaccines are derived from aborted foetal tissue and alternatives, most of which are not available in the UK. Sadly I was only made aware of the ethical difficulties involved in the manufacture of the vaccine, a few months ago, the day after my third child had received her MMR shot.
Cristina Odone wrote a particularly irksome piece yesterday, which discussed the current measles outbreak in Swansea, Wales and laid the blame squarely at the door of the middle-classes who, Odone argues, believe that their offspring are more precious and special than everyone else’s and so don’t vaccinate. The article displayed, to my mind, some unacceptable class prejudice, lampooning middle-class consumer choices as springing from a sense that they are somehow special and stating that the middle-classes secretly loved the MMR/autism scare as it validated their sense that their offspring are better than everyone else’s.
The article particularly stung for a number of reasons, not only did I recognise some of my preferred consumer choices listed, but also I was one of the parents who agonised over the decision over whether or not to vaccinate. Actually I think Cristina was entirely misguided, the reason that if I could afford to, I would shop at John Lewis, or buy the childrens’ clothes from Boden or Joules, is not because I think their products are particularly special or luxurious, they don’t pander to narcissism, but put simply, those brands tend to be understated, not especially flashy (although in the case of children’s clothes, distinctive) but mainly because they are of good quality and so last. One knows that John Lewis’ customer service is of a consistently high standard, they stand by their guarantees and treat customers well; likewise with the children’s clothes retailers, products tend to have a much longer shelf-life than their cheaper alternatives. So in the case of the children, a piece of clothing bought 9 years ago, is still in pristine condition on its 4th baby. Nothing to do with whether or not I feel my children to be special, it’s more a question of economy.
There were other unfair generalisations (both to middle and working classes) such as stating that the middle class tend to prevent their children from taking risks, and they were more likely to read or talk to their children and nurture them intellectually or feed them the requisite 5 a day portions of fruit and veg. Whilst its true that income can sometimes be a barrier to eating healthily, it doesn’t automatically follow that those on low incomes do not give their children a good diet or neglect to read or talk to them. Having money is no indicator of ability to be a good parent, this is an attitude that should be challenged.
Most parents, regardless of social class, believe their children to be special and wish to protect them from harm. All of us were alarmed by the MMR scare, which received widespread national publicity. Whilst every activity in life carries innate risks, in the case of immunisations, one is having to actively undertake a risk balancing exercise – taking one’s child to be injected requires one to be pro-active, in the sense of having to make the appointment and undertake the journey to the doctors. I suggest that this is one of the reasons behind the decline in the vaccine uptake, particularly in Swansea which isn’t noted for being an affluent middle-class area. Parents need to be wholly convinced that this is the right decision for their child, the newborn baby jabs are scheduled between the ages of 8 and 16 weeks, when one is in the post-natal baby haze, checking the baby every 2 minutes and it’s easy enough for the health visitor or midwife to jolly one off to the clinic, especially when the diseases vaccinated against are as serious as meningitis. It’s every parent’s instinct to want to protect their child from harm and thus most people don’t need much persuasion when it comes to vaccinating their fragile little newborn.
By the time the child has reached 13 months, the age at which MMR is administered, equilibrium has been recovered. People need active encouragement that there is an imperative to vaccinate. For people of my generation, who remember having mumps and German Measles as children, these diseases seem of little consequence, despite the fact we are told, that they have now mutated into something much nastier. The success of the MMR vaccine hinges solely on the fear of measles, which can have devastating effects, especially if one’s immune system is already compromised in some way. My sister had measles as a child and almost died by all accounts. For most parents it’s the risk of measles, versus the risk of the MMR and so passivity or procrastination often seems the best option.
With the withdrawal of the patents for the single vaccines, parents now have very little option, it’s either all or nothing. Whilst the arguments against the single vaccines are valid, i.e. it requires mutliple appointments which most parents don’t attend and there is the risk that a child could catch one of the diseases between vaccinations, to my mind, the government’s decision to remove this choice seems authoritarian and spiteful. No-one is demanding that the NHS gives single jabs, but there was no need to remove the option for private patients. For those who might argue about the difficulties of multiple appointments, I would argue that anyone who is concerned enough to seek out the option of single jabs, will not be taking a slapdash attitude towards their child’s health. Single jabs might well have reduced the severity of the outbreak – we’ll never know.
Andrew Wakefield has been thoroughly humiliated and discredited, but that does not mean that parents who decide against MMR should be vilified as selfish or ignorant. There are still legitimate concerns about MMR, in that many parents have horrifying testimony of the immediate effects of the vaccination upon their child, such as temporary paralysis. From my perspective, all of my children have been absolutely fine in the long-term, but they have all been extremely fractious and ill-tempered in the aftermath. But then again, when the MMR is administered, it’s not on its own. They get the MMR in one thigh and the Hib, Pneumococcal (PCV), and Meningitis C in the other. So that’s 6 doses of vaccine all in one dose. No-one is suggesting that it’s not safe, however all vaccination is counter-intuitive and it seems a heck of a lot to inject into a little 12 or 13 month old child, who may not even be walking. When my eldest had her MMR booster, aged 5, she described how it stung and burned as it went into her. Apparently that’s a common sensation. So it’s pretty tough on parents who have to watch their child receiving a painful injection, hoping that its going to protect them from a much worse evil, and yet knowing that many people believe this to be harmful. Most of us pray that it’s going to be alright and not cause them any ill-effects in the short term, though it’s hard when your child is spiking a temperature as a direct result of their immunisations.
As Catholics, we are not statists, we don’t believe that the government or state can dictate the precise healthcare or education of our chidden. The story of my eldest’s vaccinations is a cautionary tale. Shortly before they were due to be administered I read about the thiomersal scare, in one of the newspapers. Thiomersal being the mercury based preservative, which was being linked to nerve damage and autism. (This has since been discounted in a study). I therefore specifically requested that my child received Thiomersal free injections. The Health Visitor agreed and made note, informing that since I had requested this, then my daughter would receive the vaccines. What would have happened had I not requested, I asked. “She would have received the version with the thiomersal in”, said the Health Visitor. “This is being phased out, we are switching to the new Thiomersal free vaccine, but we need to use up our stocks, so we are only giving out the new version to those who specifically ask”. Furthermore, when my eldest was vaccinated as a baby, she was given a 3-in-1 injection. This has now been ramped up to a 5-in-1, together with a separate dose of PCV. As I said, it seems like a lot of pathogens to be loading onto a delicate 8 week old immune system, especially when babies can vary so much in terms of size and weight.
Understandably, the authorities charged with public health take a utilitarian attitude towards the population. Most children will be alright as a result of their vaccinations and they stress that we have a civic duty to protect the weakest. That’s all very well and good, but what when it’s your child who is the one affected, as people claim they have been?
We shouldn’t rush to pillory those who don’t vaccinate their children, or try to label them (I’m guilty of this, I live in Green Brighton which has a very low uptake) because though passivity is often the easiest course of action when faced with a dilemma (it’s easier to do nothing), I know of many highly intelligent, well educated and medically literate folk who have not vaccinated. It is impossible to make a fully informed choice because as @battlementclare, a qualified midwife notes, “there have been no rigorous long term studies into the effects of hyper stimulating the immature neonatal immune system with multiple foreign antigens & adjuvants known to be neurotoxic. I have to wonder whether, in protecting children against some diseases, we are increasing their likelihood of developing auto immune disorders later.” This is all true, the decision to vaccinate centres around a balancing of risks, with the additional factor that there are ethical problems inherent for Catholics in using vaccines derived from aborted foetal cell lines.
One can’t actually do right for doing wrong on this issue, my feeling has been to vaccinate, not least due to living in areas which have experienced measles outbreaks, but every time it has been with a heavy heart. After all no-one, regardless of their social class, (I suspect many of Cristina’s middle class stereotypes would probably fall into the new ‘precariat ‘ in any event) wants to inject their child with something that they have heard on the news or read in the newspapers, or anecdotally from a friend, could do their child harm. This is what Andrew Wakefield tapped into quite so successfully.
But on another note, Cristina’s article, irritating as it was, carries lessons for those of us fighting to get our point of view acknowledged and acted upon, in areas such as pro-life or the defence of marriage. It initially made me very angry as I perceived myself to be the object of undisguised scorn and contempt, identifying a little with some of her use of consumer brands, and having once being described as “all white teeth and Boden”. I guess I experienced some of what same sex couples feel when they read various pieces of unkind polemic, such as that written by notorious journalists or unkind bloggers, attacking people and their motivations, by virtue of their lifestyle. It’s a reminder to us all to play the ball, not the man, if we’re talking about why marriage shouldn’t need to change, there is no need to launch into a personal attack upon people of goodwill.
The same applies with abortion. Whilst we should always condemn the act, we need to understand and engage with the reasons behind abortion, as well as exercise understanding and compassion to those women who have aborted, instead of casting scorn, doubt and shame upon their motivations or lifestyle, particularly if we wish them to engage and have a conversion of heart. Just like Cristina’s piece on MMR, instead of considering the very good reasons that exist when it comes to vaccination, I was left feeling defensive for having worried about it, angry and not inclined to think well of Odone. It was highly counter-productive.
Ultimately every single parent is well aware of their child’s flaws or shortcomings, but we still love them fiercely and protectively no matter what and want to keep them safe from harm, whether we are members of the royal family, or on the very margins of society. Every parent is entitled to think their child is special, it’s called love and is what keeps the world turning. I’m sure there’s a metaphor about God in there somewhere.
All white teeth, Boden and ‘middle class’, but not a piece of rocket in sight… “The Vicar’s Wife gives her kids fruit shoots”!
There’s a fabulous phrase from Blackadder goes Forth, that would make for a very witty inscription on a tombstone and which I employ on frequent occasions when discussing pro-abortion advocates. Uttered by General Melchett (Stephen Fry before he manifested the symptoms of irrepressible smugness) whilst discussing the progress of the Great War, he tragically and comically sums up the attitude of those directing the war, thus:
If all else fails, a total Pig-Headed unwillingness to look facts in the face will see us through
I’m thinking in particular of the continued propagation of the idea that Catholic dogma played its part in the death of Savita Halappanavar, and the insistence that a timely abortion would have saved her life.
I’m going to spell this out very simply for the terminally hard of understanding.
Sunday 21st October 2012.
Savita was admitted to Galway University Hospital. She was suffering from backache and during the day had experienced some distressing blood and fluid loss. The hospital took bloods and examined her. The blood results that would have indicated that she had an infection were never followed up on, and Savita did not manifest obvious signs of infection. Sepsis is a deadly disease with a rapid progression which medical staff need to be hyper-vigilant about when dealing with pregnant women. Its symptoms can easily be masked by other symptoms in pregnancy, such as backache, raised temperature and generally feeling unwell. Savita had a history of back problems and had herself misdiagnosed her pain earlier in the day.
Savita would appear to have been suffering from a Urinary Tract Infection, (UTI) which are very common in pregnancy, need antibiotics to treat them, but are not necessarily life threatening. Let’s add into the mix that University College Hospital Galway, was over-stretched in terms of staffing and resources, this report in 2011 names it as the worst performing hospital in Ireland for the second consecutive month with calls for the Health Minister to intervene. The hospital seems to have been suffering from chronic shortages, which is something we should bear in mind before pointing the finger.
There is no reason at this point, to believe that Savita needed an abortion, let alone that her life might be at risk.
Upon examination it appears that Savita’s membranes are bulging and her cervix can’t be felt, meaning that a miscarriage is sadly imminent. There is no reason to believe that she is at risk of infection or that she needs an abortion. Later on, in the early hours of Monday morning, her membranes rupture. Again, there is no need to think that she may need unnecessary surgery, this seems like a regular miscarriage.
Monday 22nd October 2012
By 10pm on that evening, Savita’s waters had been ruptured for a full 22 hours. She was on antibiotics every six hours. It’s not clear when these were started, it should however have been from the moment the membranes ruptured and ideally based on the results of the blood culture taken on Sunday evening.
Tuesday 23 october 2012
At 8.20 am Savita is seen by Dr Astbury who informed her that ‘that the legal position in Ireland did not permit me to terminate the pregnancy in her case at that time.’ Savita is, at that point very distressed and requesting an abortion to put an end to her ordeal. No-one can blame her. She knows that she is miscarrying her baby and wants the whole thing to be over.
My take on this, is that Dr Astbury obviously sympathises. I think that she doesn’t want to take personal responsibility, or appear harsh and uncaring, nor does she want to cast the hospital in a bad light, there is no medical reason, or so it would seem, for an abortion, this isn’t life or death, they probably didn’t have a theatre or staff available at short notice and so she fell back on the letter of the law as an explanation. It’s fair to say that the law would not allow for an abortion in these circumstances, the foetal heartbeat is present, the patient seems comfortable and stable and no doubt many of the staff would have felt uncomfortable, given that this was not medically necessary, but it seems that there was no discussion as to why the hospital were taking the conservative management approach, one that would be taken in hospitals around the world. Hospitals do not deliver pregnant women the moment their membranes rupture, they can very often be sent home to get some rest in comfort, before being readmitted within the next 48 hours, depending on protocols and individual circumstances. It seems very remiss that Dr Astbury explains this in such a perfunctory and legalistic way. Surely Savita was owed more of an explanation?
If there was a clinical need for an abortion, why did Dr Asbury not consult with any of her colleagues? In any event, Savita was described as being “upset, but not unwell”.
Later on Dr Astbury testified that had she had access to Savita’s blood results earlier, then she would have taken theraputic intervention, i.e, an abortion, earlier. So how does this delay in terms of diagnosis and identifying the infection, equate with being the fault of Catholicism or uncertainty surrounding the legal situation?
But what does not make sense, is that if an infection is present or suspected, it is a contraindication for surgery – why invade a sterile uterus with instruments and risk flooding the body with further infection? Conservative management is always the default option in the treatment of miscarriages.
Wednesday 24 October 2012
This is the day that things begin to unravel for poor Savita. At 7am her pulse is 160 per minute (normal resting heart rate is usually between 60 and 80). Her blood pressure is 100/60 mm (normal is 120/80). Her temperature is 39.6 and in addition foul smelling discharge is present, suggesting infection. The doctor on duty concurs she is suffering from probable sepsis.
An hour and half later, 8.25 am, Dr Astbury and team see Savita on their ward rounds. Swabs are taken to determine what exact infection is present. According to the Irish Times, Dr Astbury testifies thus:
At this point her temperature had come down to 37.9 degrees and her pulse to 144bpm. She said she discussed with Ms Halappanavar the concern that she had inflamed foetal membranes due to infection.
“I also informed Ms Halappanavar that if we did not identify another source of infection or if she did not continue to improve we might have no option but to consider a termination regardless of the foetal heart.”
Mr Halappanavar has said he had no knowledge this discussion had taken place. In his statement he said he was at the hospital with his wife throughout Wednesday.
Subsequent to this, Savita deteriorates further, Dr Astbury consults with a colleague who agrees that delivery is medically necessary, a scan confirms that the baby has died, she is taken into theatre where she delivers, is subsequently transferred to HDU and then ICU and dies following further subsequent deterioration just after midnight on Sunday 28 October 2012.
Savita’s husband has no recollection of the conversation that a termination might be needed regardless of the presence of a foetal heartbeat.
Let’s leave aside the comments from the midwife, who was discussing abortions in a cultural context, Ireland’s Catholicism in relation to India’s Hinduism, in response to Savita’s request for an abortion. These obviously do not dictate care. Also Savita’s request for abortion should not be considered a factor. Patients’ wishes, whilst often taken into account, do not dictate what is best medical practice, as I learnt when I was refused the option of being able to deliver my youngest baby naturally. The doctors understood, they sympathised, they could see I was distressed and terrified and they did what they could to help me be comfortable, but ultimately they would not agree to the course of action that I requested, because it was deemed to be unsafe, and interestingly more unsafe for the baby than for me. I could not force them to act against my best medical interests.
Why would an abortion be required if the Dr could not find the source of the infection? It is clear that the baby could not have been the source of the infection. This is biologically impossible. A baby would not suddenly become infected and pass this onto the mother. The baby is in a sterile environment, even after the membranes have ruptured. The inflamed foetal membranes referred to, or to give it the correct medical term, chorioamnionitis, had not been identified. If this was the concern, which would require delivery, why wasn’t this possibility examined for sooner? It all seems like amateur guesswork. Finding the source of the infection, and treating the infection is a wholly different issue as to why the baby would need to be delivered. Plus we know that Savita presented with infection at the hospital, prior to the rupture of the membranes.
And here’s the absolute crunch. Four key failures. The blood test results performed on Savita on the Sunday evening admission, were ready at 6.37pm that evening, but not read until 5.25pm the next day. They were not then accessed again until after sepsis had been diagnosed and Savita’s condition was rapidly deteriorating, two days later. When Savita started shivering at 4.15am on the Wednesday morning, the first obvious signs that sepsis was raging through her body, her vital signs should have been checked. They were not. The blood culture sample taken from Savita at 8:29 am on Wednesday 24th October was processed onto the computer system by microbiology at 9.54 am but not reviewed by Dr Astbury until 11:20am. The lab also reported that the 2nd key sepsis test should have been performed on the ward, it was not. This a lactate serum test which could have definitively confirmed the presence of sepsis. The sample was taken at 6am on the Wednesday morning and stored in an inappropriate bottle before being sent to the lab who could not process it. The lab would not, in any event have carried out this test which should have been performed at a point of care unit on the ward.
The antibiotic treatment administered to Savita between 7am and 1pm was ineffective as it was erythromycin, a variant that is resistant to E-coli, the infection that pathology determined killed her. Broader spectrum antibiotics would have been a better choice.
The indications that Savita had sepsis were subtle and overlooked, by staff who were not deliberately negligent, but who were overstretched and under-resourced.
Catholics and pro-lifers have been writing today of the horrors of Kermit Gosnell. Pro-choicers have been calling his case an exception from which no broader conclusions can be drawn. Why then, in the case of Savita Halappanavar, and in the face of all evidence to the contrary in this one-off extraordinary case, under which Irish law allowed for an abortion, are they claiming that this is evidence that the law is causing women to die in droves?
Savita died from an E.coli infection, which the likelihood is, entered her urinary tract and bloodstream, causing her to miscarry. It was this bacteria that killed her and prompt identification of it, along with the correct antibiotics that could have saved her life. Aborting her baby would have made no difference to the progress of the disease and would have risked further infection and hastened death.
As well as holding the hospital to account, Parveen should be asking questions of the pro-choicers who have chosen to cynically exploit this tragedy for their own ends. The baby did not kill Savita, the E.Coli did.